Jordan’s national response to HIV/AIDS is characterized by a strong and significant political commitment. There is an increasing awareness and political commitment at all levels, resulting, for example, in the participation of government officials and members of the Royal Family in advocacy efforts.
Jordan, through extensive collaboration and coordination between all interested parties, succeeded in achieving the three main requirements to scale up toward universal access, which are known as The Three Ones. They are:
1) One agreed HIV/AIDS Action Framework that provides the basis for coordinating the work of all partners – defined as the NAS mentioned in the previous section.
2) One National AIDS Coordinating Authority that has a broad-based, multi-sectoral mandate as defined as the CCM.
3) One agreed country-level monitoring and evaluation system. Recently, Jordan has adopted a Monitoring and Evaluation plan which has been developed by the National AIDS Programme (NAP) with technical and financial support from United Stats Agency for International Development (USAID) primary through Family Health International (FHI). This plan, include well defined indicators for all activities implemented by NAP.

The UNAIDS and World Health Organization (WHO) global report for 2007 estimates 0.02% HIV sero-prevalence in the adult Jordanian population (WHO/UNAIDS 2006), thus classifying Jordan as a low prevalence country comparing to the global HIV/AIDS epidemic. Several factors have been observed which may either mask a higher HIV prevalence, or contribute to an accelerated future spread of the epidemic. These factors include low levels of awareness, high levels of stigma and discrimination against PLHIV and marginalization of most-at-risk populations such as sex workers.
Data collected in 2006 and 2007 shows a 31% increase in the cumulative number of HIV/AIDS cases reported in Jordan. The total number of HIV/AIDS reported cases is currently 548, compared to 426 in 2005. This number represents all cases reported in Jordan since the first case was reported in 1986. As this data is recorded through passive case reporting, and rarely through the voluntary utilization of Voluntary Counseling and Testing (VCT) services, it may not necessarily provide an accurate reflection of national HIV prevalence. For example, little is known about prevalence among vulnerable populations in Jordan; although formative assessments of vulnerable populations are planned under the 2005 National HIV/AIDS Strategy (NAS). Greater awareness among high risk populations brought about by targeted prevention programming may have contributed slightly to a rise in the number of Jordanians seeking VCT. However, there is consensus that a low level of awareness in the general population, the misconceptions surrounding the virus and the marginalization of high-risk groups may be camouflaging a higher HIV prevalence. Factors that may contribute to a further spread of the epidemic include economic hardships resulting from the sharp increase in the cost of
living, high levels of mobility related to refugee migration from neighboring countries in conflict situations, and to high levels of labor migration to and from Jordan, as well as the increase in risky behaviors among young people including increased drug use.

in a low prevalence epidemic setting. Jordan's NAS (2005-2009) has classified most-at-risk groups into primary and secondary, based on their degree of vulnerability. Primary groups include Female Sex
Workers (FSW), Men who have sex with men (MSM) and Injecting Drug Users (IDU); while secondary groups consist of youth, frequent travelers, military service personnel, workers in certain sectors (health, tourism and transport), prisoners ,refugees and street children.
Information on injecting drug users is also limited, though some data is available on drug use in general. Two studies concerning drug use in Jordan were conducted by UNODC in the past few years. The Global School Health Survey (GSHS), developed by the World Health Organization (WHO) in collaboration with UNICEF, UNAIDS, UNESCO and the Centre for Disease Control and Prevention
(CDC) was disseminated to 2471 students. Official results of the study were presented in August 2005. The study found that students in Jordan are not invulnerable to drug use, with 3% responding in a positive manner. The second study conducted was the UNODC "Rapid Assessment Situation on Drug Abuse and Dependence in Jordan”, published in 2001. In this survey more then 5000 students in the age group between 18 and 25, mainly university (80%) and community college students (20%), were interviewed with regard to their patterns of drug use, including alcohol, tobacco and sedatives. The major substances used or abused by the respondents (last month prevalence) were: tobacco (29%),
sedatives (12%) and alcohol (12%].
As for vulnerable groups classified as secondary in the NAS, some surveys among youth have been conducted. In a survey of 3000 young people, 3.3% of males and 0.6% of females had had a non-regular sexual partner in the previous 12 months and, among that group, condom use was 40.3%. (NAP, 06)In a survey of 8800 households conducted in May 2001, it was reported that 6.6% of young people knew a peer who had sniffed glue, gas or paint; 2.5% knew someone who had taken tranquilizers, codeine or morphine; 1.3% knew of someone who had used hallucinogens; and 0.4% knew someone who had used cocaine. Although there were no questions on sexual behavior, general sexual knowledge was poor, as demonstrated by the fact that more than half of the young people (60%) knew no typical features of physical changes in puberty (UNICEF, 2002).
Also among secondary populations are workers in the tourism industry. USAID supported qualitative research, primarily through FHI that involved 70 in-depth interviews, among tourist workers in Petra (Drew, 2004). Key findings included widespread beliefs that it is possible to tell a person with HIV/AIDS by sight that tourists are screened for HIV and that Jordan is HIV-free and a poor knowledge of STIs, as well as a strong distrust of public health services and reports of commercial sexual activity among tourists and tourist workers.
These information doesn’t show the follow up for people who got infected with HIV and if they had families or they were responsible for kids and they became orphaned because of their parents getting infected. it does seem that we have a really serious problwm regarding the awareness of the transmition methods and the admition of sexual activity before marriage. As a conservative culture it would be honest to say that it is not acceptable to have sex before getting married , maybe that’s why the statistics is not that reliable here in Jordan because of the stigma about HIV.
So what am trying to say is the STIGMA issue about HIV , homo sexual , is a really big thing in our culture . and a major problem we have is that sexual and reproductive health in general is extremely POOR and need to be focused on specially among the up coming generations.




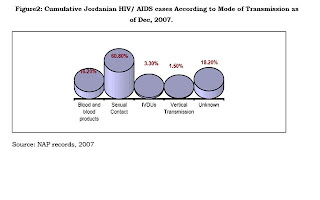
These graphs show the lack of social information about HIV and its related issues from stigma to sex workers to the homosexual , it is really something that we suffer from , that no body reports about their condition or about what is happening with them , am not saying that every body do this , but it is the majority , despite the fact that because of the relatively conservative culture we have low incidence of HIV among other countries , at least that’s what graphs shows !!.
